Pharmacotherapeutic Group: Drugs for dementia,
ATC code: N06DA02.
Pharmacology: Pharmacodynamics: Donepezil HCl is a specific and reversible inhibitor of acetylcholinesterase (AChE), the predominant cholinesterase in the brain. Donepezil HCl is
in vitro over 1000 times more potent an inhibitor of this enzyme than of butyrylcholinesterase, an enzyme which is present mainly outside the central nervous system.
Alzheimer's Dementia: In patients with Alzheimer's dementia participating in clinical trials, administration of single daily doses of Aricept Evess 5 or 10 mg produced steady-state inhibition of AChE activity (measured in erythrocyte membranes) of 63.6% and 77.3%, respectively when measured post-dose. The inhibition of AChE in red blood cells by donepezil HCl has been shown to correlate changes in ADAS-Cog, a sensitive scale which examines selected aspects of cognition. The potential for donepezil HCl to alter the course of the underlying neuropathology has not been studied. Thus, Aricept Evess cannot be considered to have any effect on the progress of the disease.
Efficacy treatment with Aricept has been investigated in 4 placebo-controlled trials, 2 trials of 6-month duration and 2 trials of 1-year duration.
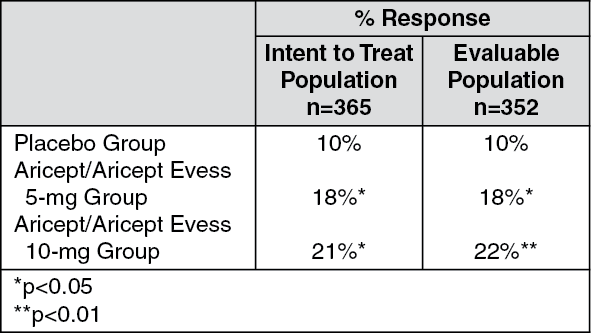
In the 6-month clinical trial, an analysis was done at the conclusion of donepezil treatment using a combination of 3 efficacy criteria: The ADAS-Cog (a measure of cognitive performance), the Clinician Interview-Based Impression of Change (CIBIC) with Caregiver Input (a measure of global function) and the Activities of Daily Living Subscale of the Clinical Dementia Rating Scale (a measure of capabilities in community affairs, home and hobbies and personal care).
Patients who fulfilled the criteria listed as follows were considered treatment responders. (See table.)
Response: Improvement of ADAS-Cog of at least 4 points.
No deterioration of CIBIC.
No deterioration of Activities of Daily Living Subscale of the Clinical Dementia Rating Scale.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Aricept Evess produced a dose-dependent statistically significant increase in the percentage of patients who were judged treatment responders.
Pharmacokinetics: Absorption: Maximum plasma levels are reached approximately 3-4 hrs after oral administration. Plasma concentrations and area under the curve (AUC) rise in proportion to the dose.
The terminal disposition half-life (t
½) is approximately 70 hrs, thus, administration of multiple single-daily doses results in gradual approach to steady state. Approximate steady state is achieved within 3 weeks after initiation of therapy. Once at steady state, plasma donepezil HCl concentrations and the related pharmacodynamic activity show little variability over the course of the day.
Food did not affect the absorption of donepezil HCl.
Distribution: Donepezil HCl is approximately 95% bound to human plasma proteins. The plasma protein-binding of the active metabolite 6-
O-desmethyldonepezil is not known. The distribution of donepezil HCl in various body tissues has not been definitively studied. However, in a mass balance study conducted in healthy male volunteers, 240 hrs after the administration of a single 5-mg dose of
14C-labeled donepezil HCl, approximately 28% of the label remained unrecovered. This suggests that donepezil HCl and/or its metabolites may persist in the body for >10 days.
Metabolism/Excretion: Donepezil HCl is both excreted in the urine intact and metabolised by the cytochrome P-450 system to multiple metabolites, not all of which have been identified. Following administration of a single 5-mg dose of
14C-labeled donepezil HCl, plasma radioactivity, expressed as a percent of the administered dose, was present primarily as intact donepezil HCl (30%), 6-
O-desmethyl donepezil (11%, the only metabolite that exhibits activity similar to donepezil HCl), donepezil-cis-
N-oxide (9%), 5-
O-desmethyl donepezil (7%) and the glucuronide conjugate of 5-
O-desmethyl donepezil (3%). Approximately 57% of the total administered radioactivity was recovered from the urine (17% as unchanged donepezil) and 14.5% was recovered from the faeces, suggesting biotransformation and urinary excretion as the primary routes of elimination. There is no evidence to suggest enterohepatic recirculation of donepezil HCl and/or any of its metabolites.
Plasma donepezil concentrations decline with a t
½ of approximately 70 hrs.
Sex, race and smoking history have no clinically significant influence on plasma concentrations of donepezil HCl. The pharmacokinetics of donepezil has not been formally studied in healthy elderly subjects or in Alzheimer's patients. However, mean plasma levels in patients closely agreed with those of young healthy volunteers.
Patients with mild to moderate hepatic impairment had increased donepezil steady-state concentrations; mean AUC by 48% and mean C
max by 39% (see Dosage & Administration).
Toxicology: Preclinical Safety Data: Extensive testing in experimental animals has demonstrated that donepezil HCl causes few effects other than the intended pharmacological effects consistent with its action as a cholinergic stimulator (see Overdosage). Donepezil HCl is not mutagenic in bacterial and mammalian cell mutation assays. Some clastogenic effects were observed
in vitro at concentrations overtly toxic to the cells and >3000 times the steady-state plasma concentrations. No clastogenic or other genotoxic effects were observed in the mouse micronucleus model
in vivo. There was no evidence of oncogenic potential in long-term carcinogenicity studies in either rats or mice.
Donepezil HCl had no effect on fertility in rats and was not teratogenic in rats or rabbits, but had a slight effect on still births and early pup survival when administered to pregnant rats at 50 times the human dose (see Use in pregnancy under Precautions).


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out
